There are two forms of gastric bypass surgery – Roux-en-Y gastric bypass surgery (RYGB) and single anastomosis gastric bypass, which is also known as Omega-Loop or ‘Mini’ gastric bypass (MGB) surgery. Both procedures are performed through laparoscopic (keyhole) surgery, but there are advantages and disadvantages to each technique that make each suitable for different people.
What is the difference between a Roux-en-Y Gastric Bypass and a ‘Mini’ Gastric Bypass?
MGB is a newer form of gastric bypass surgery. A long, narrow stomach pouch is formed through surgical stapling and attached to the small bowel. This anastomosis (surgical join) bypasses approximately two metres of small bowel. In comparison, RYGB requires two anastomoses and is a more complicated procedure.
Roux-en-Y gastric bypass surgery
 Roux-en-Y gastric bypass surgery has been around for more than 30 years. The procedure has two parts:
Roux-en-Y gastric bypass surgery has been around for more than 30 years. The procedure has two parts:
Part One: Stomach Pouch
The surgeon divides the stomach into a large portion and a much smaller one. Then, in a process sometimes called “stomach stapling,” the small part of the stomach is sewn or stapled together to make a pouch, which can hold only a cup or so of food.
With such a small stomach, people feel full quickly and eat less. This strategy is also called “restrictive,” because the new stomach size restricts how much food it can hold.
Part Two: Bypass
The surgeon disconnects the new, small stomach pouch from the majority of the stomach and first part of the small intestine (the duodenum), and then connects it to a part of the small intestine slightly farther down (the jejunum). This surgical technique is called a “Roux-en-Y.”
After a Roux-en-Y, food passes directly from the stomach into the jejunum, bypassing the duodenum. This curbs your absorption of calories and nutrients. This weight loss method is called “malabsorptive.”
Stomach stapling and Roux-en-Y are typically done during the same surgery and together are called a “Roux-en-Y gastric bypass.”
Advantages
- Effectiveness: It is one of the most effective weight loss procedures, with patients losing more weight after a gastric bypass than after a gastric band, and equal weight loss to that of sleeve gastrectomy.
- Good results with health complications: Gastric bypass effectively resolves obesity-related health problems including rapid resolution of type 2 diabetes in 80 per cent of patients by the time they are discharged from hospital, long before significant weight loss occurs.
- Good results with reflux: It is the best weight loss option for people with severe pre-existing gastro-oesophageal reflux disease, especially those with Barrett’s oesophagus.
- Long term data: Gastric bypass has a proven track record. It has been the most commonly performed weight loss operation in the United States for last 20 years and long-term results are available.
Disadvantages
- Technical complexity: The RYGB is more invasive and complex than a MGB, gastric band or sleeve gastrectomy. It carries a higher risk of post-operative complications and long-term nutritional deficiencies and therefore requires more frequent monitoring to identify and manage complications early.
- Potential for serious side effects: A RYGB carries the risk of developing complications down the track (such as dumping syndrome, peptic ulcers and internal herniation of the bowel), which do not occur after a gastric band or sleeve.
Mini-Gastric Bypass
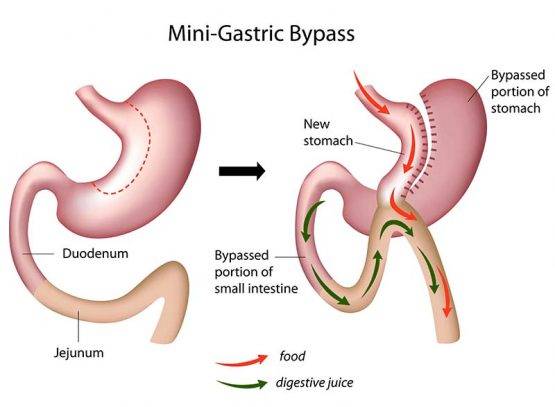 The Mini-Gastric Bypass or single anastomosis gastric bypass, is an effective and well-established procedure which combines some of the properties of a gastric sleeve and a standard gastric bypass. The upper part of the stomach is divided into a tube, similar to the top three quarters of a sleeve, and then joined to a loop of intestine.
The Mini-Gastric Bypass or single anastomosis gastric bypass, is an effective and well-established procedure which combines some of the properties of a gastric sleeve and a standard gastric bypass. The upper part of the stomach is divided into a tube, similar to the top three quarters of a sleeve, and then joined to a loop of intestine.
The mini-gastric bypass can be used as a primary weight loss procedure. It can also be used in patients who have had previous gastric banding or sleeve surgery but have been unsuccessful with weight loss, or who have had band-related complications and have decided on revision surgery.
Advantages
- Less technical complexity: This theoretically reduces the risk of an anastomosis leak.
- Theoretically reduced risk of internal hernias: As there is a single anastomosis, there is only one potential site for abnormal protrusion (herniation) of bowel.
- Shorter operative time: The single anastomosis technique is faster to perform, and is theoretically easier to reverse or revise if required.
- Safe and effective alternative: Studies comparing MGB to RYGB report that it is an appropriate alternative, and has similar results with weight loss and recovery.
- Good results with type 2 diabetes: Studies have reported that MGB is an effective form of treatment for type 2 diabetes.
Disadvantages
- The potential for more serious side effects: The surgical pathway created in MGB permits reflux of bile (digestive juice). This persistent bile reflux can cause ulceration, which leads to concerns about the long term risk of stomach or oesophageal cancer, however long term studies have not yet been performed. Patients with symptomatic bile reflux may also require reversal of their bypass, or to have their MGB converted to a standard RYGB.
- Vitamin and mineral deficiencies: As a larger portion of small bowel is bypassed in MGB, individuals are at greater risk for nutritional deficiencies following surgery.
- Long term data is not available for MGB: as a newer procedure, MGB lacks the breadth of research regarding long term outcomes that RYGB possesses.