45Kg and 58 weeks after surgery … I am finally No Longer Obese !!! (and I have not been down to this weight for more than 30 years)…
According to my BMI, I am officially not Obese any more … but I am still Overweight (which I guess still makes me a Fat Bastard).
About Body Mass Index (BMI)
Body Mass Index (BMI) is the most common (and simplest) way of measuring whether or not your are overweight. But in recent years, more researchers argue that it’s not the most accurate way to measure body weight. For years, scientists have said that BMI can’t distinguish between fat and muscle, which tends to be heavier and can tip more toned individuals into overweight status, even if their fat levels are low.
BMI also doesn’t take into account different types of fat, each of which can have different metabolic effects on health. BMI cannot take into consideration, for example, where the body holds fat. Belly fat, which is known as visceral fat, is more harmful than fat that is simply sitting under the skin.
Your BMI is determined by a relatively simple calculation using your height and weight. The formula is BMI = kg/ m2 – where kg is your weight in kilograms and m2 is your height in metres squared.
So my BMI is currently 88.4/1.72 2= 29.88 – which allows me to just scrape out of the Obese range (over 30) and into the overweight range (25-30)… A BMI of 25.0 or more is overweight, while the “healthy” range is 18.5 to 24.9 …so my “healthy” range is 55-74Kg (apparently)
So Why BMI ?
BMI is still the preferred way to measure weight and evaluate obesity primarily because it is a relatively easy measurement for doctors to take during an office visit. Taking a person’s height and weight and plugging it into an equation produces a number that informs doctors about whether their patients are at high, low or no risk when it comes to weight-related health problems.
Using the BMI measure alone, an athlete such as the 19yr old up and coming Broncos powerhouse prop – Payne Haas – would be considered Obese (119Kg, 194cm = a BMI of 31)
There are better ways to measure body fat … that provide more useful readings on how likely a person’s weight will contribute to chronic health problems. CT scans and MRIs can provide a clearer glimpse at the body’s make-up by separating out fat from muscle, for example. But these are expensive and involved compared to stepping on a scale.
So without a viable way to change how we measure body fat, for now, BMI is still probably the best option.
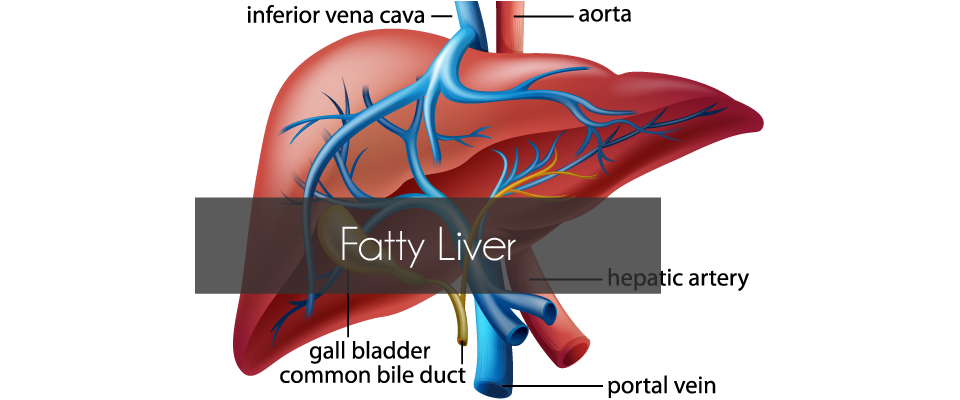
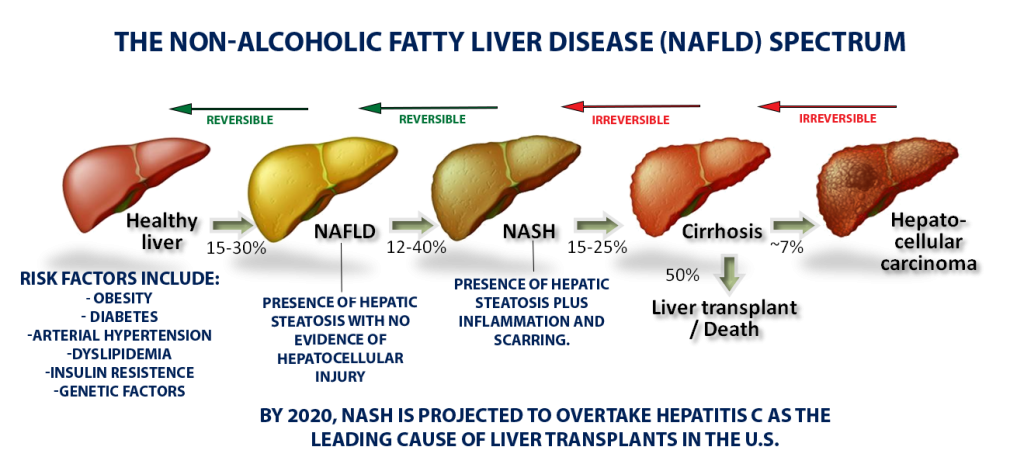
For most of us, the acronym NASH won’t ring many bells. But NASH, or NonAlcoholic SteatoHepatitis, marked by the accumulation of an unhealthy amount of fat and scar tissue in the liver, is quietly reaching epidemic proportions across the globe. By 2020, NASH is projected to overtake hepatitis C as the leading cause of liver transplants, largely because of an alarming rise in obesity and type-2 diabetes – both key risk factors for NASH.
Despite NASH’s prevalence, its obscurity isn’t all that surprising as it doesn’t cause obvious symptoms in most people, there’s no simple test to detect it, and no drugs have been approved to treat it.
Unlike high blood pressure or diabetes, which doctors can detect with cheap and easy tests during a routine check-up, NASH is difficult to diagnose. Most people with scarring on their liver don’t display symptoms, and right now there’s no straightforward biomarker that a routine blood panel would pick up. The only reliable measure of fibrosis is a liver biopsy. Also, the disease progresses slowly—over years or even decades—and researchers have yet to figure out when someone with a fatty liver is at risk for developing the inflammation and fibrosis that define NASH.
The subtle, slow-moving process begins with the build-up of fat in the liver, a condition called nonalcoholic fatty liver disease, or NAFLD, because it is not driven by alcohol consumption. For many people, a fatty liver will never become a real problem – If you have isolated fat, you may live and die with your fatty liver and never know it. But a portion of the population will go on to develop NASH’s telltale inflammation and scarring.
Anywhere from 5% to 20% of people with NASH will go on to develop cirrhosis, where scarring has stiffened the liver so much that it can no longer function properly. From there, the outcomes can be grim: liver failure, liver transplant, or liver cancer.
Right now, doctors can only recommend lifestyle changes—better diet, more exercise, less alcohol—to stop or reverse damage to the liver, which has an amazing ability to regenerate healthy cells. However, studies have shown time and again that people are unable to stick to a healthier regime, which is one reason why Bariatric Surgery (which in many ways “enforces” lifestyle changes) is considered a a viable treatment option.
One of the main reasons I went ahead with Weight Loss Surgery was to manage/control my Diabetes II. After several years of trying diet and exercise, the medications I needed to keep my blood sugar under control were increasing. I am now very happy to say that since my surgery (just over 2 weeks ago), I have stopped all diabetes medication and my blood sugar remains completely normal.
I didn’t believe I was able to manage my Diabetes by diet alone… but recent research suggest that diet drinks and artificial sweeteners (which I used to have regularly) has a link to increased risk for Diabetes II.
I am satisfied that there was no direct link with my Blood Sugar readings and consumption of diet soda (I used to have 2 and up to 6 cans of Pepsi Max a day)… These drinks are “sugar free” and I could see that my blood sugar was unaffected 1-3 hrs after consumption (whereas I could see spikes in blood sugar after eating carbs/sugary food)… However research by the Adelaide Medical School has found that high intake of low-calorie sweeteners (like those found in diet drinks) over just two weeks was enough to significantly alter the make-up of bacteria in the gut… which in turn effects the way the body absorbs and regulates blood sugar – increasing the risk of developing diabetes over time.
The researchers recruited 27 healthy subjects who were given a quantity of two different non-caloric artificial sweeteners (sucralose and acesulfame-K) equivalent to drinking 1.5L of diet beverage per day, or an inactive placebo.
The study determined that just 2 weeks of NAS supplements was enough to enhance glucose absorption and increase the magnitude of the response of blood glucose as a result. The authors conclude that “This study supports the concept that artificial sweeteners could reduce the body’s control of blood sugar levels and highlights the potential for exaggerated post-meal glucose levels in high habitual NAS users, which could predispose them to developing type 2 diabetes”.
The same Researchers are now setting out to prove for the first time if these sweeteners are actually impairing blood glucose control in type 2 diabetes sufferers rather than improving it, as has always been believed.
In the lead up to surgery I looked into lots of medical research and studies that described weight loss surgery – and in particular examined at long term benefits and effects of Bariatric Surgery.
I also spoke with a number of people who had had different types of surgery.. and others that had considered it and chosen to try traditional weight loss strategies such as diet and exercise.
Not everyone had a good outcome from the surgery… or would recommend it to others… but the majority seem to have been happy.
I discovered that not many people in my own circle of friends had experienced weight loss surgery (or were comfortable talking about it), so I found myself broadening my scope to try and talk to a wider range of people who had had experience (or knew someone who had).
I would like to broaden this even further, and would LOVE to hear from anyone reading this who is happy to share your experiences.
So if you have had any experience with weight loss – good or bad – surgery based or not.. Please go to our Your Story page and fill in whatever details you are comfortable with (you can remain anonymous if you prefer).
A British Journal of Surgery study ( indicates that weight-loss surgery is cost-effective over 10 years and can save healthcare systems money over a lifetime.
The April 2018 study found that Weight-loss surgery was associated with reduced average costs to the UK National Health Service by €2742 (£1944), and a gain of 0.8 life-years and 4.0 quality-adjusted life years over a lifetime compared with usual care. It also had the potential to reduce the lifetime risks of obesity-related cardiovascular diseases and diabetes.
“Despite increased rates of obesity in the UK, England has one of the lowest utilization rates of bariatric operations in Europe and issues with limitations in patient access to surgery,” said co-author Vasily Lukyanov, of Synergus AB, in Sweden. “The findings of the study justify non-limited access to surgery to all eligible categories of obese patients in England.”
Borisenko, V. Lukyanov, A. R. Ahmed. Cost-utility analysis of bariatric surgery. British Journal of Surgery, 2018; DOI: 10.1002/bjs.10857
I’ve been doing a lot of research into the effectiveness of Weight Loss Surgery – and in particular, the long term benefits it has to offer. All the data I have encountered (Swedish Obesity Study, US Veterans Study) highlights the significant advantages of weight loss surgery over traditional weight loss strategies (diet, exercise, counselling, support). It is largely this data which convinced me that the risk of not doing anything was much higher than the risk of the surgical option.
But I started to wonder what type of research there was about the long term effects of non-surgical weight loss strategies.
The Biggest Loser
The Biggest Loser was (once) a very popular reality TV program which followed the progress of severely obese contestants to see who could lose the most weight (for a significant prize). It started out in the USA in 2004 and ran for 17 seasons over a 12 year period. The show came to Australia in 2006 and ran for 11 seasons to 2017.
This program provides a very public glimpse into spectacular weight loss results achieved in a relatively short period, by very motivated people with lots of support, assistance and motivation. It demonstrates that massive weight loss can certainly be achieved in the short term, but offers no indication as to the long term benefits of this type of weight loss regime… In fact when you look into it a little deeper any information about long term results is noticeable by its absence. Apart form a few “guest appearences” from past contestants (usually from the previous season), there is next to no mention of how the rest are getting on.
In 2016, a study published in Obesity Journal examined the current situation of 14 contestants, 6 years after they appeared as contestants on The Biggest Loser. The focus of this study was primarily to look at long term changes in their metabolic rate.
Researchers studied 14 contestants who participated in the 30-week competition, which involves intensive diet and exercise training. They started at an average weight of 149 kg and ended at an average weight of 91 kg. Six years later, when the six men and eight women went to the National Institutes of Health for follow-up measurements :
weight, on average, was back up to 131 kg. Only one participant hadn’t regained any weight.
percent body fat started at an average of 49 percent, dipped to 28 percent and returned to 45 percent over time.
Allbutonesubjectregainedsomeoftheweightlostduringthecompetitionandfivesubjectswerewithin1%oftheiroriginal weightorabove. On average, the group regained much of their weight but did maintain about 12 percent weight loss even after six years, had better cholesterol profiles, and none had developed diabetes during follow-up.
Summary
Whilemostsubjectsexperiencedsubstantialweightregaininthe6 yearssince“TheBiggestLoser”competition,themeanweightloss was11.9%comparedwith their original baseline weightand57%oftheparticipantsmaintainedatleast10%weightloss. Incomparison :
The 2016 study found that only one of the 14 Biggest Loser contestants examined weighed less than when the competition completed, with four of them now heavier than their starting weight, and nine returning to within 10% of their previous weights. Whereas according to the Journal of Obesity outcomes for patients undergoing gastric bypass surgery are far superior, with patients losing 60-70 per cent of excess weight after a year with approximately 50 per cent of this access weight loss maintained after 15 years.



 I am satisfied that there was no direct link with my Blood Sugar readings and consumption of diet soda (I used to have 2 and up to 6 cans of Pepsi Max a day)… These drinks are “sugar free” and I could see that my blood sugar was unaffected 1-3 hrs after consumption (whereas I could see spikes in blood sugar after eating carbs/sugary food)… However research by the Adelaide Medical School has found that high intake of low-calorie sweeteners (like those found in diet drinks) over just two weeks was enough to significantly alter the make-up of bacteria in the gut… which in turn effects the way the body absorbs and regulates blood sugar – increasing the risk of developing diabetes over time.
I am satisfied that there was no direct link with my Blood Sugar readings and consumption of diet soda (I used to have 2 and up to 6 cans of Pepsi Max a day)… These drinks are “sugar free” and I could see that my blood sugar was unaffected 1-3 hrs after consumption (whereas I could see spikes in blood sugar after eating carbs/sugary food)… However research by the Adelaide Medical School has found that high intake of low-calorie sweeteners (like those found in diet drinks) over just two weeks was enough to significantly alter the make-up of bacteria in the gut… which in turn effects the way the body absorbs and regulates blood sugar – increasing the risk of developing diabetes over time.
 I discovered that not many people in my own circle of friends had experienced weight loss surgery (or were comfortable talking about it), so I found myself broadening my scope to try and talk to a wider range of people who had had experience (or knew someone who had).
I discovered that not many people in my own circle of friends had experienced weight loss surgery (or were comfortable talking about it), so I found myself broadening my scope to try and talk to a wider range of people who had had experience (or knew someone who had).
 A British Journal of Surgery study ( indicates that weight-loss surgery is cost-effective over 10 years and can save healthcare systems money over a lifetime.
A British Journal of Surgery study ( indicates that weight-loss surgery is cost-effective over 10 years and can save healthcare systems money over a lifetime.
 The Biggest Loser was (once) a very popular reality TV program which followed the progress of severely obese contestants to see who could lose the most weight (for a significant prize). It started out in the USA in 2004 and ran for 17 seasons over a 12 year period. The show came to Australia in 2006 and ran for 11 seasons to 2017.
The Biggest Loser was (once) a very popular reality TV program which followed the progress of severely obese contestants to see who could lose the most weight (for a significant prize). It started out in the USA in 2004 and ran for 17 seasons over a 12 year period. The show came to Australia in 2006 and ran for 11 seasons to 2017.